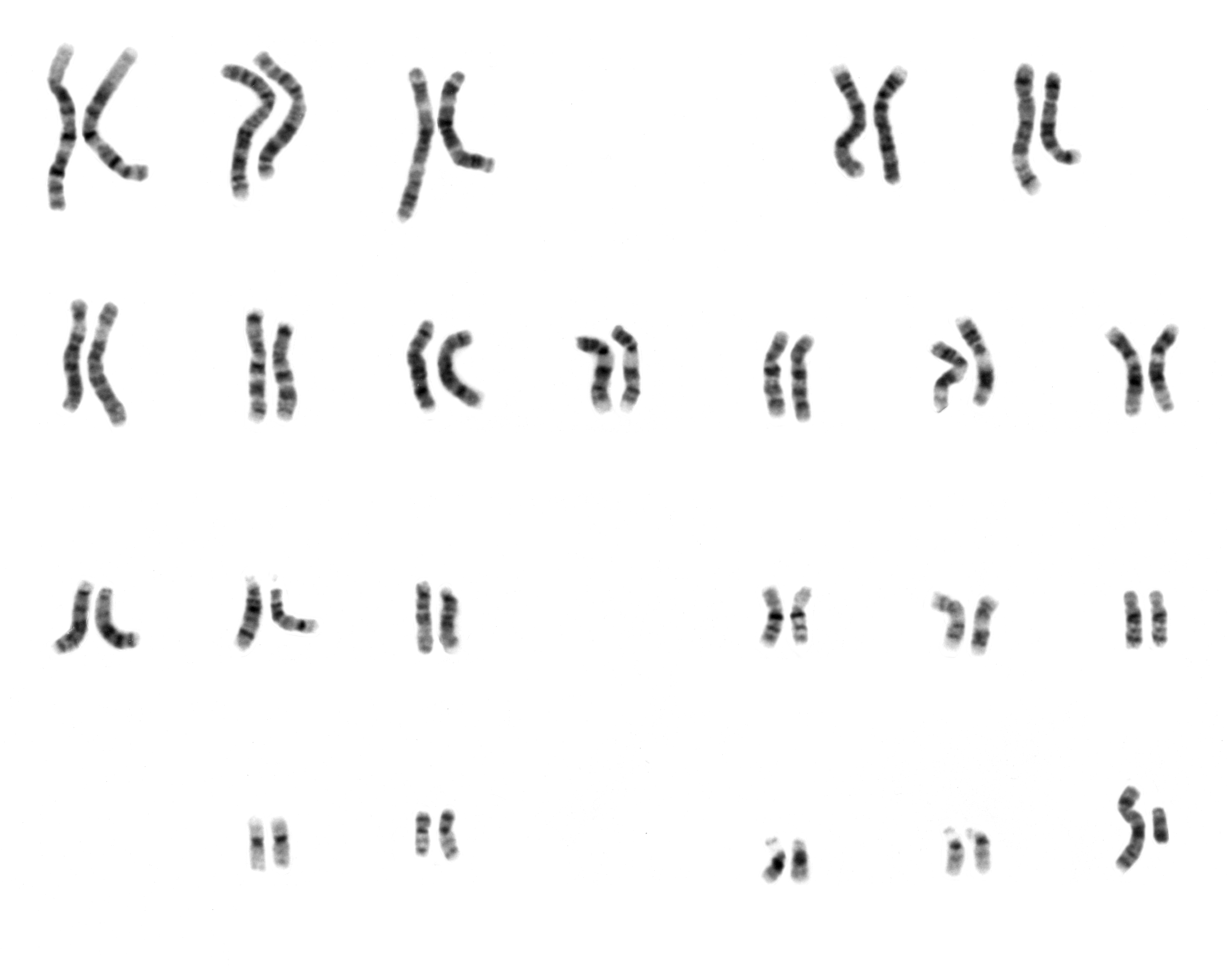

To help facilitate understanding of the changes in Clara, I will briefly go over chromosome structure (use figure below as a reference). Chromosomes have a center called the centromere which is where the two copies of the same chromosome come together prior to cell division. On each side of the centromere are the two arms of the chromosome. The shorter of the arms is called the p arm and the longer arm is called the q arm. These arms are segmented based on density of the DNA/protein (as observed through light/dark bands). The bands are labeled with the number increasing as one moves away from the centromere.

So her leukemia karyotype:
45, XX, -5, -7, add(10)(p), -11, add(11)(q23), +2mar[cp8]
What should it be? 46, XX
So what does all that mean? Her leukemia cells have 45 chromosomes (instead of 46). She is a normal XX (female). She is missing copies of 5, 7, and 11. **She has additional DNA on the p arm (the short arm) of chromosome 10 (I guess they don't know where). She also has additional DNA on part of the q arm of chromosome 11.** There are also two chromosomes that don't resemble known chromosomes (probably a mix of stuff) called marker chromosomes.
The FISH analysis indicated that there was a break at 11q23. This is a common break in leukemia in the middle of the MLL gene. They see that part of this gene (3' end) is with the additional DNA on chromosome 10 (add(10p)). This may indicate a translocation between chromosome 10 and 11 (t(10;11)) but I guess that they aren't sure or they would have labeled it so. t(10;11) translocations tend to happen in AML, but the exact location seems to matter. We know it is 11q23 somewhere in the MLL gene, but we don't know where on chromosome 10.** FISH also showed that EGR1 (a gene on chromosome 5 at a common break point) is normal and in two copies. This indicated that there isn't really a deletion of chromosome 5 but that it is probably part of the add() and/or marker chromosomes.
Missing chromosome 5 and 7 are usually linked with poorer prognosis potentially making her high risk. We have yet to hear from the doctors regarding her risk level and the last doctor seemed to indicate that she was standard risk. We will be talking to the AML expert to get a better explanation of these results in due time. If she is high risk then she is most likely going to need a bone marrow transplant.
EDIT: I made some changes between the **'s. I misunderstood what add() indicated and have corrected this.
3 comments:
phew. thanks for the explanation, Alan. Must admit that i was beginning to think I wasn't going to decipher it - but by the end I get exactly what you meant! (thanks for allowing me to feel a little smarter with your good layperson translation!)
I hate to think of the meaning of the markers, because I want her to stay in the standard risk category - but glad that you can research to this level and be able to question the prognosis with the AML expert. Please keep us informed.
sending my best positive thoughts and prayers every day. Love you guys!
Hi Alan.
I sent this link to the head of our cytogenetic lab and she came back with a lengthy response. I understand if you do not want outside opinions cluttering the issue but if you want I will forward it to you. Email me at gbowden@ggc.org. We are praying for you all. Good luck.
Greg Bowden
I'm so glad you are reading the blog, Greg! You know that I know you and Alan are doing similar work in genetic labs/research..(even though I don't understand any of it)
And each time I read of these high vocabulary word lists in posts I think maybe you understand some of it too?
So I'm glad to see you are reading and now posting too!
Alan-I'm trying to follow you as best as I can. I remember you trying to explain your research paper that one Christmas. I listened as hard as I could the whole time. I think I'm just as lost. But I'm listening! And I'm glad you are keeping us all informed. Maybe I will understand what I've listened to eventually;). Maybe I'll practice re reading it every day.
Lauren
Post a Comment